🔄 The Bi-Directional Axis: Type 2 Diabetes and MASLD
Fatty liver disease and Type 2 Diabetes Mellitus (T2DM) are not merely comorbid conditions—they are two sides of the same metabolic coin.
For years, clinicians viewed hepatic fat accumulation as a passive consequence of metabolic syndrome. Today, advanced pathophysiological insights reveal an aggressive, bi-directional loop: diabetes accelerates liver damage, while a fatty liver worsens insulin resistance, creating a self-perpetuating metabolic cycle.
Here is a look at the mechanics of this axis and why unified screening protocols are crucial for patient care:
📊 The Stark Clinical Reality
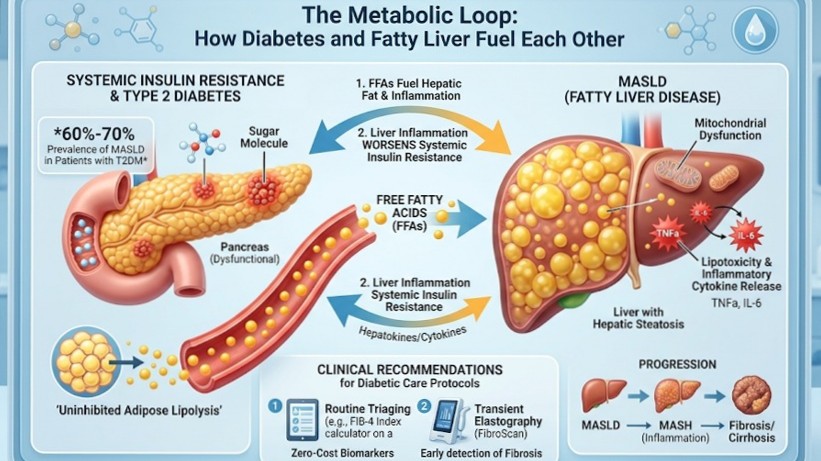
The epidemiological overlap between these two conditions is massive. Clinical data reveals that over 60% to 70% of patients living with Type 2 Diabetes also have concurrent MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease).
More alarmingly, when a patient has both T2DM and MASLD, the risk profile changes dramatically. Diabetes acts as an independent accelerator, significantly increasing the likelihood of progression from simple steatosis to active MASH (Metabolic Dysfunction-Associated Steatohepatitis), severe fibrosis, cirrhosis, and hepatocellular carcinoma.
🔄 Inside the Loop: The Pathophysiological Mechanism
How do these two conditions fuel each other? The driver is chronic insulin resistance.
1. Dysregulated Lipolysis: In an insulin-resistant state, adipose (fat) tissue becomes resistant to insulin's normal "storage" signals. This triggers uninhibited lipolysis, causing a massive, continuous release of Free Fatty Acids (FFAs) into the bloodstream.
2. Hepatic Influx & Lipotoxicity: The liver acts as a sink, absorbing this overwhelming influx of circulating FFAs. The liver converts these into triglycerides, leading to hepatic steatosis. Over time, these lipids accumulate as toxic intermediates, triggering cellular stress, mitochondrial dysfunction, and localized inflammation (MASH).
3. Compounding Resistance: As the liver becomes increasingly engorged with fat, it produces higher levels of inflammatory cytokines and hepatokines. This directly worsens systemic insulin resistance, making blood glucose management progressively harder for the pancreas and creating a closed, destructive loop.
🩺 Clinical Recommendations: Shifting to Routine Screening
Because early-stage MASLD and even progressive fibrosis are frequently asymptomatic—often hiding behind completely normal liver enzyme panels (ALT/AST)—we cannot afford a reactive approach. Screening for liver disease must become a routine component of standard diabetic care protocols.
• Primary Triaging (The FIB-4 Index): Every patient with Type 2 Diabetes should undergo routine risk stratification using non-invasive biomarkers. The FIB-4 Index is a simple, zero-cost calculator utilizing a patient’s age, AST, ALT, and platelet count to rule out advanced fibrosis.
• Secondary Evaluation (Transient Elastography): Patients identified as indeterminate or high-risk through secondary blood biomarkers or ultrasound should be escalated for a FibroScan. This measures hepatic stiffness and fat accumulation accurately, allowing for early, protective clinical intervention before structural damage becomes irreversible.
🤝 A Multi-Disciplinary Mandate
Breaking this metabolic loop requires active collaboration across clinical specialties. By integrating routine hepatology triaging into diabetology and endocrinology practices, we can identify high-risk individuals early, optimize metabolic treatments, and alter the trajectory of chronic liver disease.